RADIA: Beyond DICOM AI for Medical Imaging in Fundoscopy & Ultrasound
When a fundus image reveals 5 retinoblastoma foci in seconds, or a Doppler ultrasound identifies a 40 mm hypervascular mass with a complete clinical differential — the question stops being "can AI do this?" and becomes "how were we not using it before?"
Most medical AI platforms focus on a single niche: chest CT, digital mammography, or bone X-rays. But the reality for healthcare professionals is far more diverse. An ophthalmologist needs to analyze fundus photographs looking for signs of glaucoma or intraocular tumors. A musculoskeletal radiologist reviews Doppler ultrasounds to differentiate a hemangioma from a sarcoma. A rural physician wants a second opinion on that fundus image they just captured with a portable retinal camera.
RADIA was born as a DICOM viewer with AI for CT and dental CBCT, but its multimodal architecture — four AI models analyzing each image in cascade — works equally well with any clinical image. Today we show how it processes two modalities that go far beyond classic DICOM: fundus photography (retinography) and soft tissue ultrasound with color Doppler.
2 modalities, 11 cases, 0 missed findings
In the tests documented in this article, RADIA correctly identified multicentric retinoblastoma (5 tumor foci), severe papilledema with urgent neuroimaging recommendation, ischemic retinopathy with cotton wool spots, and hypervascularized soft tissue masses with complete clinical differential — all with confidence levels above 90%.
Fundus Photography: The Retina as a Clinical Window
Retinography — fundus photography — is one of the most informative and least invasive tests in medicine. Through the dilated pupil, a camera captures the retina, optic disc, macula, and retinal vessels. In that single image, dozens of pathologies can be detected: from diabetic retinopathy and glaucoma to intraocular tumors and signs of intracranial hypertension.
The problem is that interpreting a fundus photograph requires specialized experience. A primary care physician may not recognize a cotton wool spot or might confuse a benign nevus with a choroidal melanoma. RADIA tackles exactly this problem: the AI analyzes each image with the same systematic approach as an experienced retinologist, identifying findings, classifying them by severity, and suggesting clinical differentials.
Pigmented Macular Lesion — Nevus or Melanoma?
The first case shows a fundus photograph with a pigmented oval lesion in the macular region, temporal to the optic disc. This is the type of finding that can trigger immediate alarm — is it a benign choroidal nevus or an early melanoma?
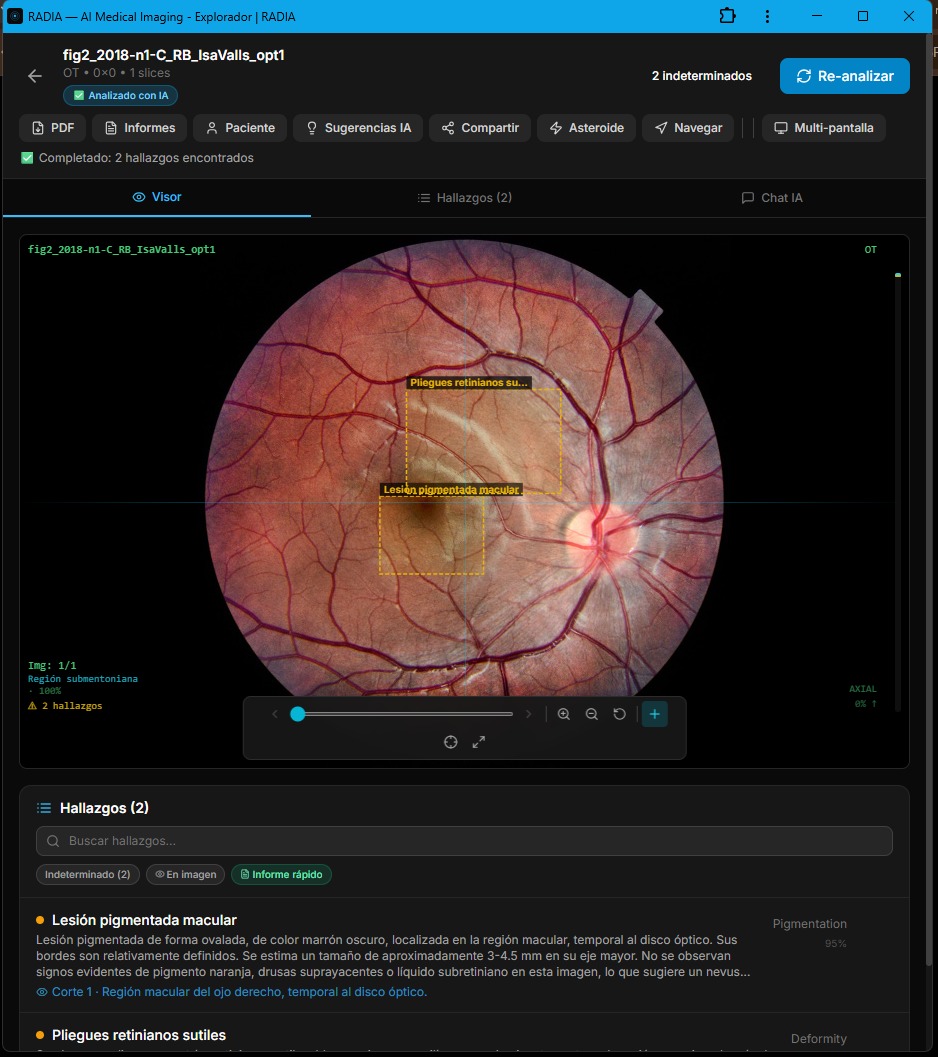
RADIA identified two findings:
Pigmented macular lesion
Oval pigmented lesion, dark brown color, located in the macular region, temporal to the optic disc. Borders are relatively well-defined. Estimated size: 3-4.5 mm in its major axis. Category: Pigmentation 95%.
Subtle retinal folds
Presence of subtle folds in the retina surrounding the lesion, suggestive of traction or minor deformity of retinal tissue. Category: Deformity.
What's relevant here isn't just the detection — any trained eye sees the dark spot. What matters is the categorization. RADIA doesn't say "malignant tumor" when it isn't. It classifies the findings as indeterminate, notes the absence of orange pigment, overlying drusen, or subretinal fluid (markers of malignant transformation), and suggests a benign choroidal nevus as the most probable finding. That precision avoids unnecessary referrals and patient anxiety.
Multicentric Retinoblastoma: 5 Tumor Foci in Seconds
Retinoblastoma is the most common malignant intraocular tumor in childhood. Detecting it early can save not only the eye but the child's life. And when it's multicentric — multiple independent foci — the urgency multiplies.
In this case, RADIA analyzed the image with Asteroid Mode (deep multi-model analysis) and detected 5 malignant findings, all classified as Neoplasm with 98% confidence.
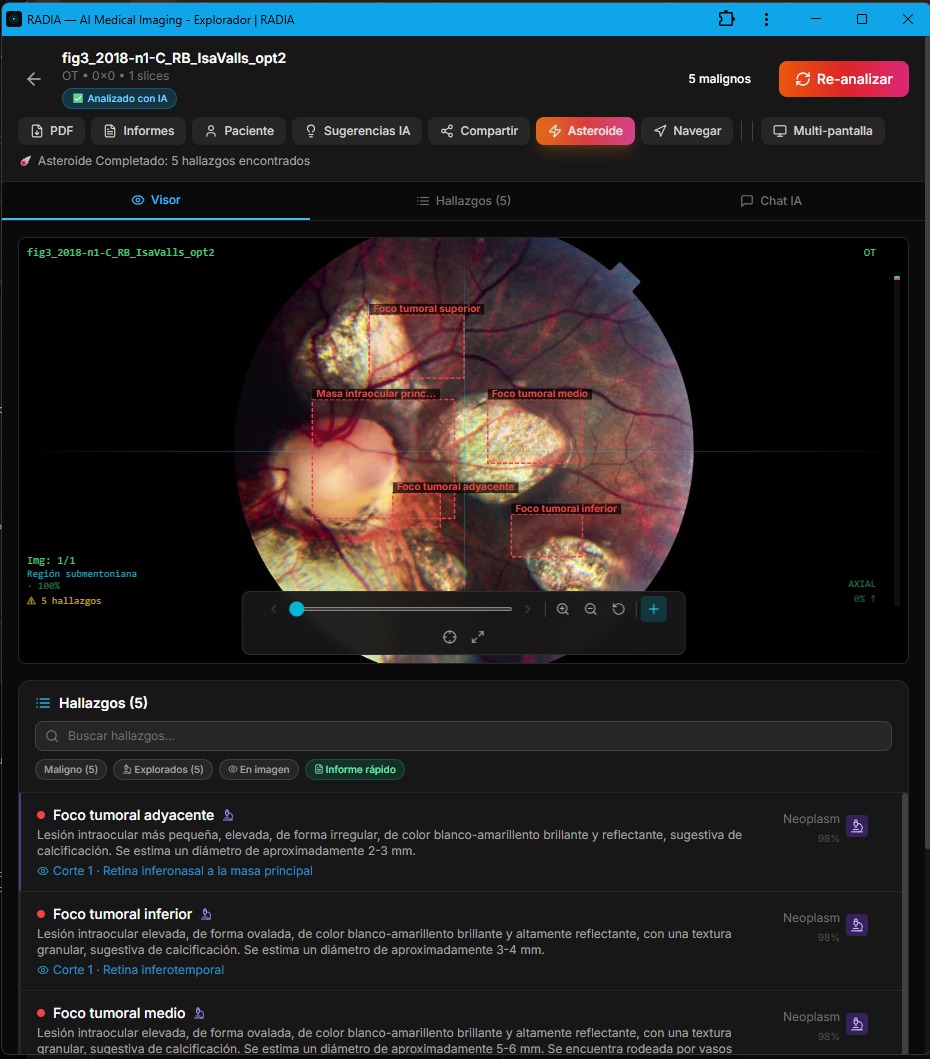
The 5 detected findings
| Finding | Est. size | Location | Confidence |
|---|---|---|---|
| Main intraocular mass | Large mass | Posterior pole | 98% |
| Adjacent tumor focus | 2-3 mm | Inferonasal retina | 98% |
| Inferior tumor focus | 3-4 mm | Inferotemporal retina | 98% |
| Middle tumor focus | 5-6 mm | Mid retina | 98% |
| Superior tumor focus | 2-3 mm | Superior retina | 98% |
Each focus was described individually: "elevated intraocular lesion, bright white-yellowish and highly reflective, with a granular texture suggestive of calcification." The presence of calcification is the most specific marker of retinoblastoma on imaging, and RADIA identified it in all foci.
Why does this matter?
Multicentric retinoblastoma requires a different therapeutic strategy than unicentric. Detecting all 5 foci — including the smallest ones at 2 mm — can change the decision between intra-arterial chemotherapy and enucleation. Automated screening at this level in primary care would mean earlier referrals and better outcomes.
Papilledema: When the Eye Reveals a Brain Problem
Papilledema is optic disc swelling caused by intracranial hypertension. It's a neurological emergency diagnosed by looking inside the eye. Brain tumors, venous sinus thrombosis, pseudotumor cerebri — all can first manifest as a blurred, elevated optic disc on fundoscopy.
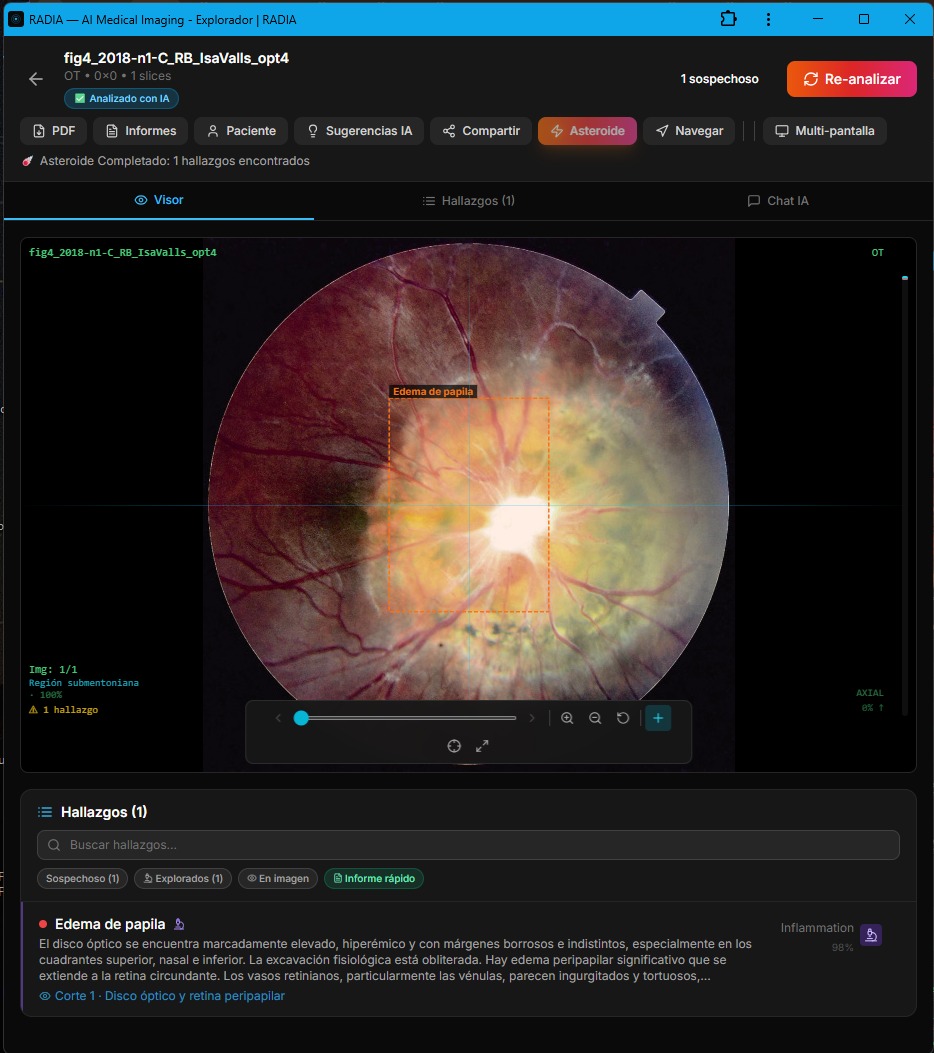
RADIA described the finding with clinical precision: "markedly elevated optic disc, hyperemic with blurred and indistinct margins in all directions, especially in the superior, nasal, and inferior quadrants. The physiological cup is obliterated. Significant peripapillary edema extending into the surrounding retina."
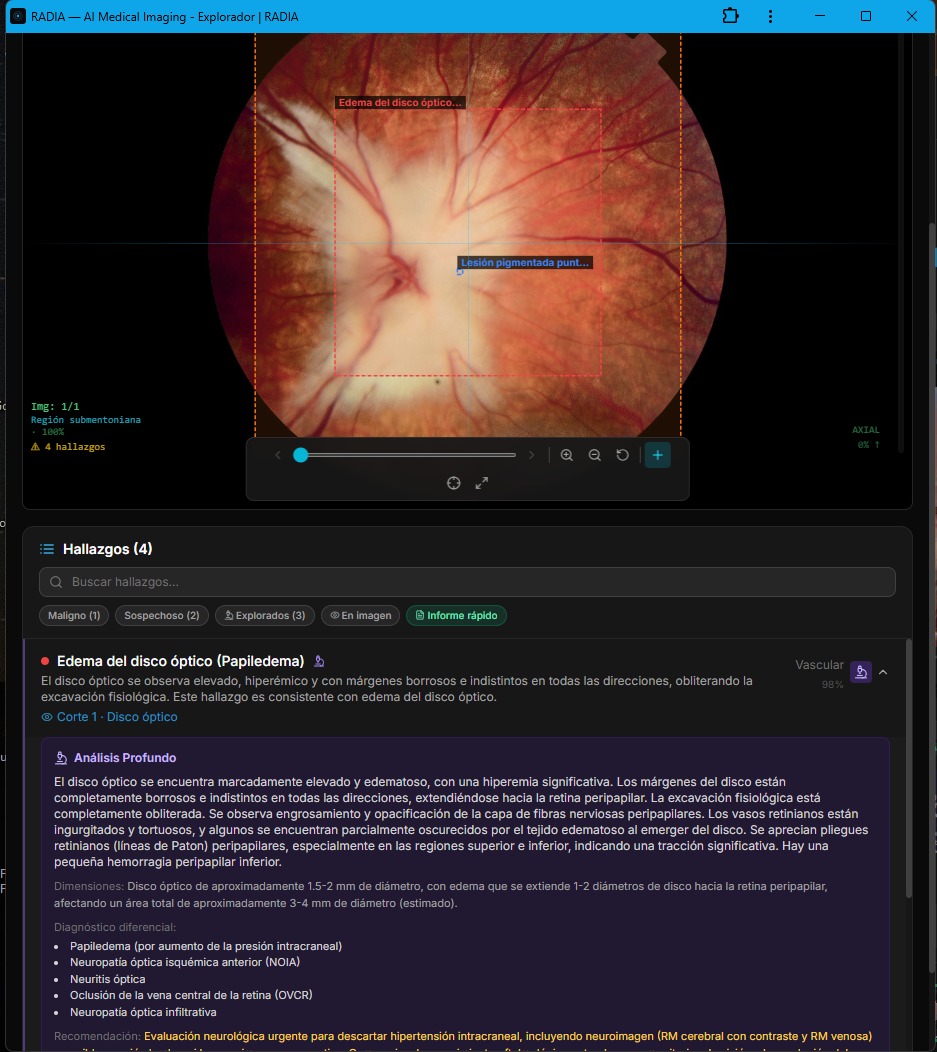
The Deep Analysis included a complete clinical differential:
AI-generated clinical differential
And most importantly: the red-highlighted recommendation — "Urgent neurological evaluation to rule out intracranial hypertension, including neuroimaging (contrast-enhanced brain MRI and venous MRI)." RADIA doesn't just detect, it prioritizes. A finding requiring urgent neuroimaging is flagged as such, never lost among data.
Severe Ischemic Retinopathy: Multiple Simultaneous Findings
This case is the most complex in the ophthalmology set. A fundus photograph showing diffuse vascular changes, cotton wool spots, papilledema, and retinal hemorrhages — all in the same image. It's the kind of case that demands analyzing multiple interrelated findings and synthesizing a coherent clinical picture.
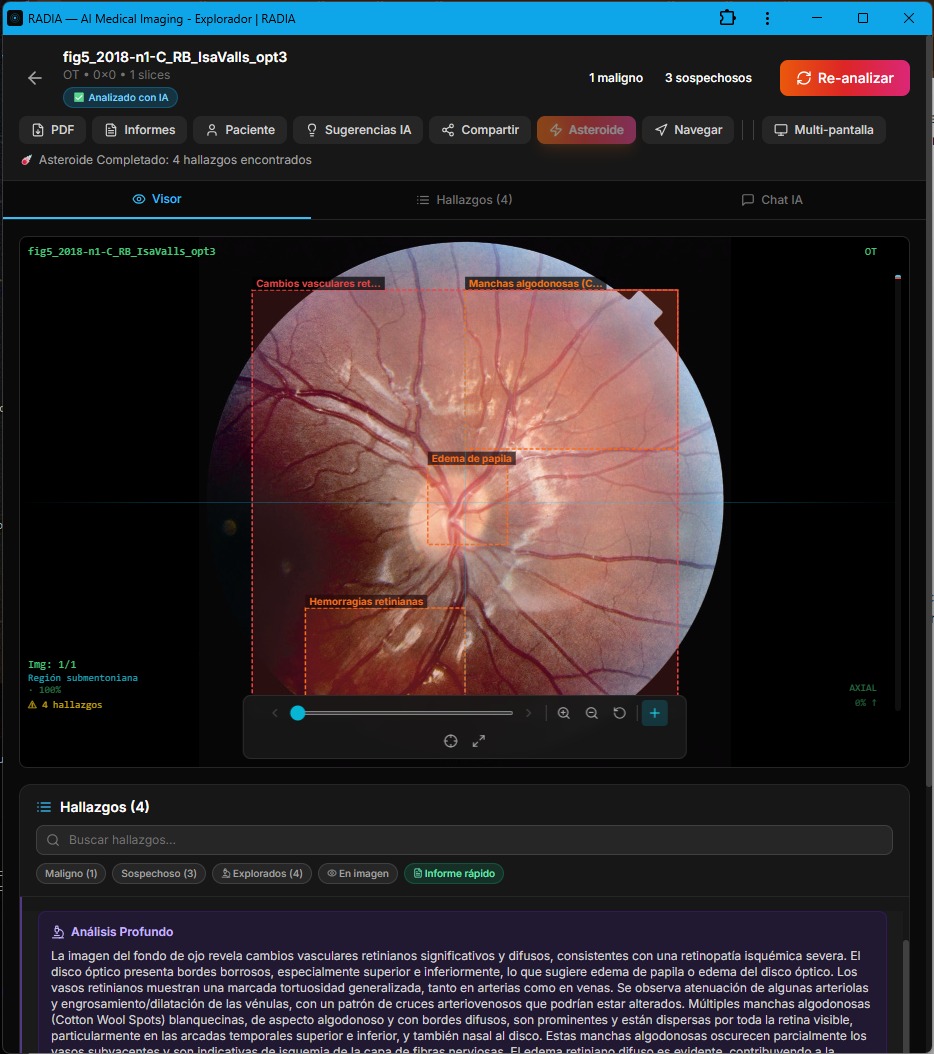
Retinal vascular changes
Generalized vascular tortuosity, arteriolar attenuation, venular engorgement. Arteriovenous crossings with altered pathological pattern.
Cotton Wool Spots
Multiple whitish lesions with diffuse borders scattered across the visible retina, indicative of nerve fiber layer ischemia.
Papilledema
Optic disc with blurred margins, generalized edema. May indicate associated intracranial hypertension or ischemic neuropathy.
Retinal hemorrhages
Dot and blot intraretinal hemorrhages located in the inferotemporal quadrant.
The AI synthesized all these findings into a coherent clinical picture: "severe and diffuse retinal microangiopathy, consistent with ischemic retinopathy." The clinical differential included severe/malignant hypertensive retinopathy as the leading option. This isn't a list of isolated findings — it's integrated clinical reasoning.
PointAsk: "What do you see here?" — Click, Ask, Answer
One of RADIA's most powerful features is PointAsk: the doctor clicks on any point in the image and the AI specifically analyzes that area. Not a general analysis — a focal analysis at the exact coordinates the professional points to.
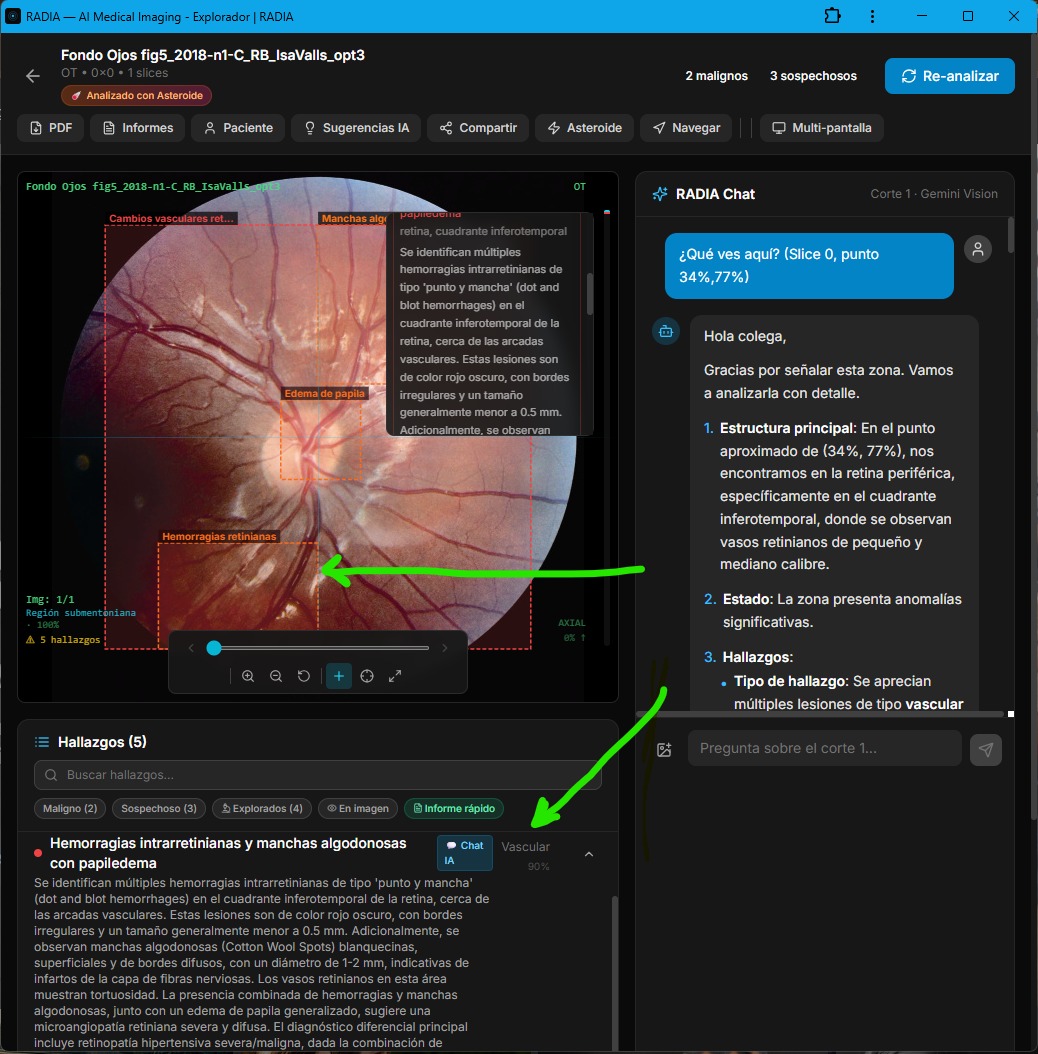
In this screenshot, the user asked "What do you see here?" by clicking on the inferotemporal quadrant of the retina. The AI responded with a detailed structure:
Main structure
Peripheral retina, inferotemporal quadrant, small and medium caliber retinal vessels.
Status
The area shows significant abnormalities.
Findings
Multiple vascular-type lesions: dot and blot intraretinal hemorrhages, cotton wool spots of 1-2 mm indicative of nerve fiber layer ischemia.
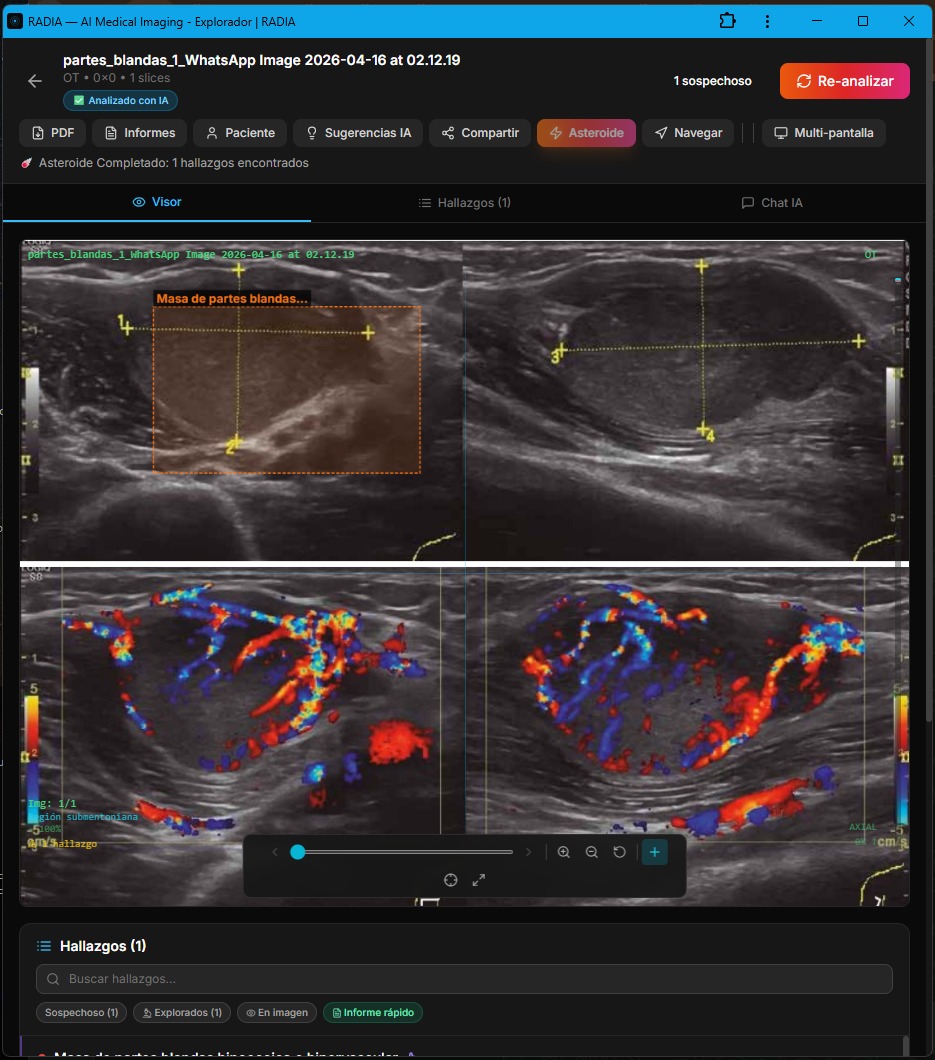
Soft Tissue Ultrasound: Doppler, Masses, and Clinical Differential
Soft tissue ultrasound is the first-line study for palpable masses in the neck, extremities, and subcutaneous tissue. When color Doppler is added, the information multiplies: you see not only the shape and size of the lesion, but its vascularity — and that's what separates an innocent lipoma from an aggressive sarcoma.
The following three cases show how RADIA handles Doppler ultrasounds natively, extracting dimensions, vascular pattern, echogenicity, and generating clinical differentials that a musculoskeletal radiologist would validate.
Hypoechoic Hypervascular Mass — 25×40 mm
A palpable soft tissue mass. B-mode ultrasound shows a well-defined, predominantly hypoechoic lesion with an oval to lobulated shape. So far, it could be anything. But color Doppler reveals massive hypervascularization — tortuous, abundant vessels with high-energy arterial and venous flow.
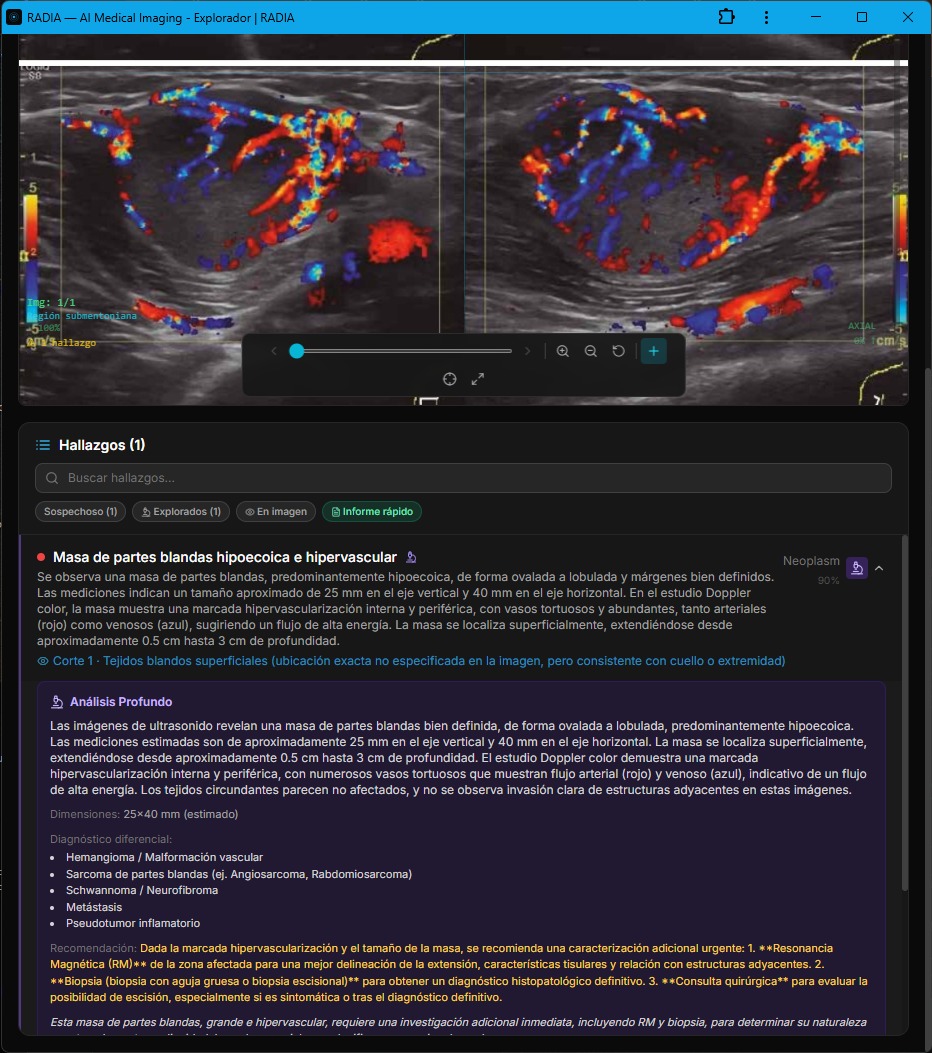
AI-generated clinical differential
The recommendation was clear and highlighted: MRI of the affected area for better delineation + core needle or excisional biopsy for definitive histopathological diagnosis. RADIA doesn't leave the doctor with a "suspicious finding" — it provides the concrete next step.
Hypervascular Superficial Soft Tissue Mass — Neoplasm 95%
This case shows two views of the same lesion on color Doppler. The upper image presents an intensely hypervascular mass — a rainbow of red, orange, and blue indicating mixed high-velocity arterial and venous flow. The lower image offers another perspective with a visible scale.
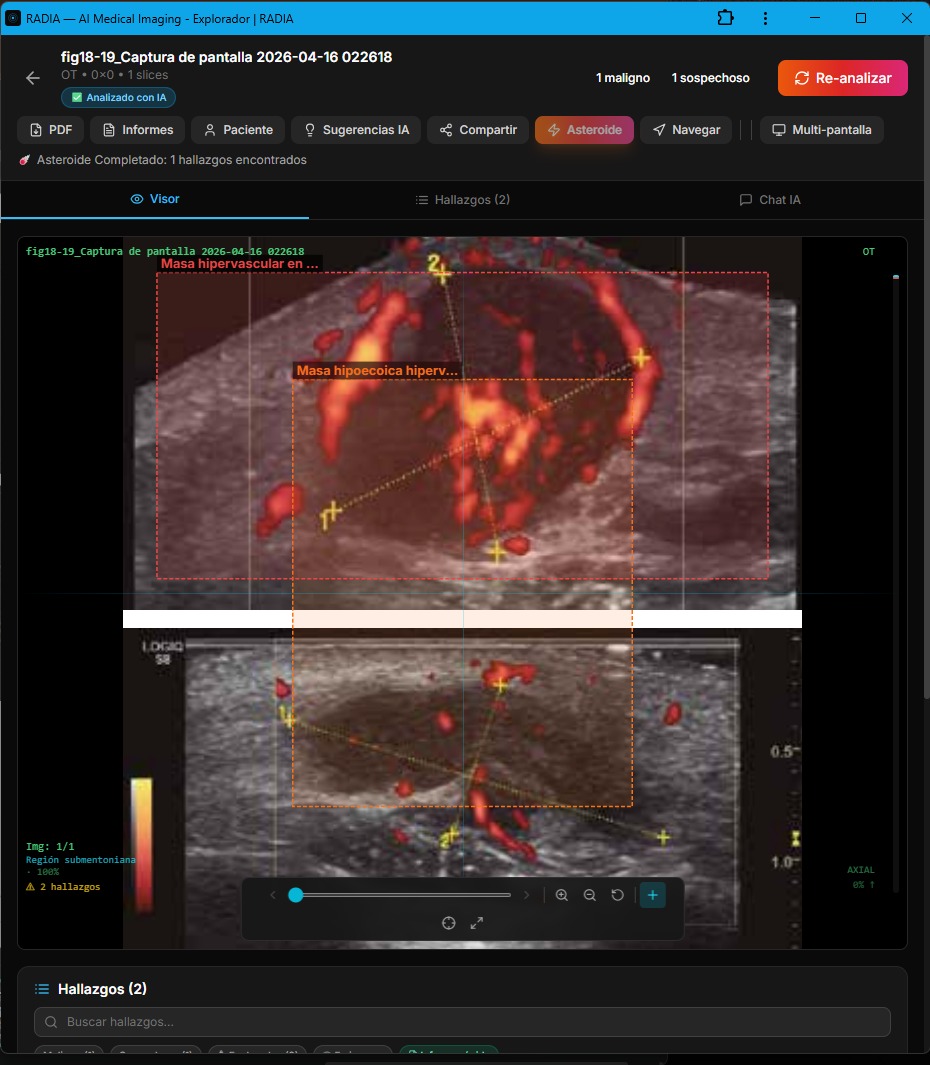
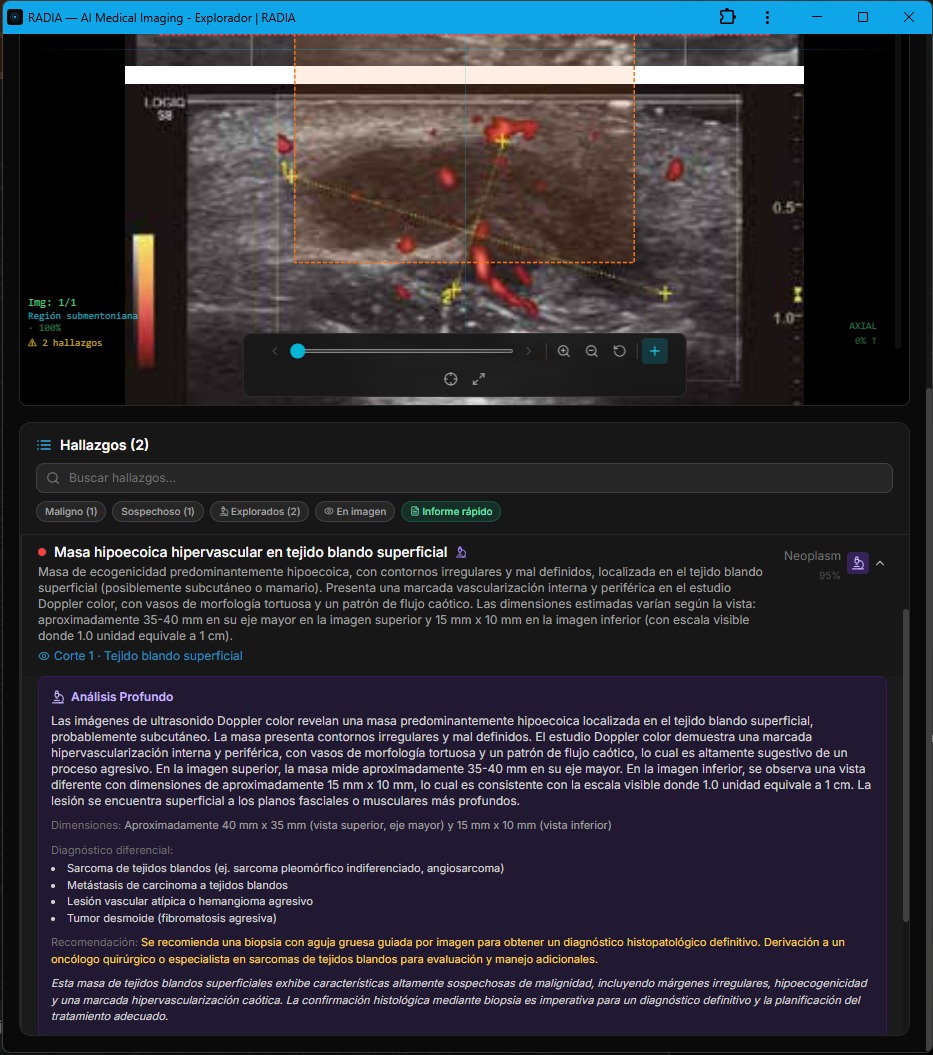
RADIA measured the mass in both views: 35-40 mm × 35 mm in the upper and 15 mm × 10 mm in the lower (visible scale 1.0 unit = 1 cm). It detected irregular contours, tortuous vascularization with a chaotic flow pattern — characteristics "highly suggestive of an aggressive process."
Clinical differential — Case 6
Recommendation: image-guided core needle biopsy + referral to surgical oncologist or soft tissue sarcoma specialist.
Complex Cystic Lesion — 45×20 mm with Internal Septa
Not everything RADIA detects is malignant. This case shows a complex cystic lesion in subcutaneous tissue — predominantly hypoechoic to anechoic, with multiple thin internal septa and some punctate echoes. No significant internal vascularity on B-mode. Size: 45-50 mm wide by 20-25 mm deep.
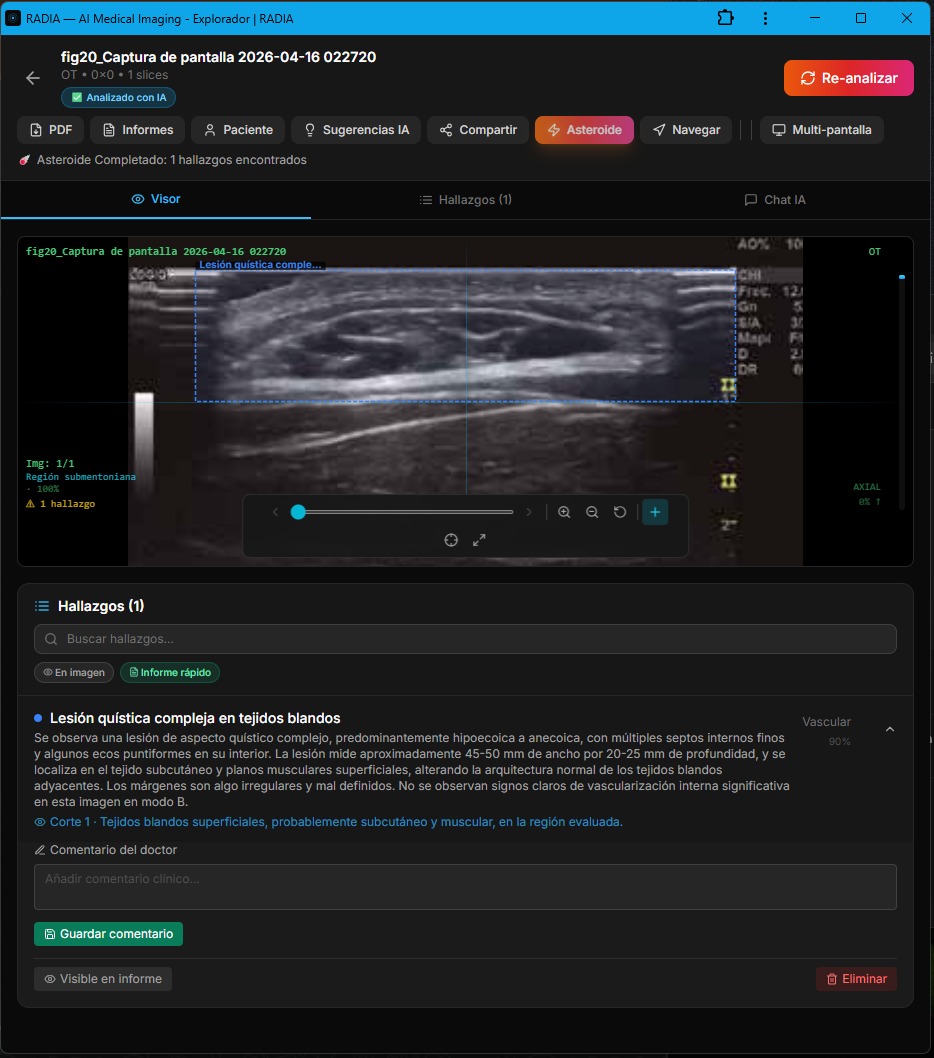
The AI classified this finding with Vascular 90% confidence and noted that the margins are somewhat irregular but there are no signs of significant internal vascularity — reducing malignancy suspicion. The screenshot also shows the "Doctor's comment" field, where the professional can add their clinical impression directly on the finding before generating the report.
This case illustrates the importance of AI not over-diagnosing. Not all masses are malignant tumors. A complex cyst requires follow-up but not the urgency of a hypervascular sarcoma. RADIA differentiates between both scenarios with precision, avoiding the cascade of unnecessary tests that a false positive generates.
How It Works: From Pixel to Finding
Behind every finding there's an AI pipeline processing the image in multiple layers. It's not a single model — it's four AI models working in cascade.
Upload & normalization
The doctor uploads the image (JPEG, PNG, DICOM). RADIA normalizes it, extracts metadata and generates thumbnails for fast navigation. For DICOM studies, the viewer offers progressive HQ rendering: instant scrolling with 8-bit PNG, and when paused for 800ms it loads the original DICOM at 16-bit with full dynamic range. All in the browser.
Multi-model AI analysis
Gemini 2.5 Flash (general analysis + clinical reasoning), MedGemma 4B-IT (specialized medical model) and Llama 4 Scout (cross-validation) process the image in parallel. DeepSeek Reasoner applies chain-of-thought reasoning over findings as a Clinical Council.
Structured extraction
Models return structured JSON with findings, bounding box coordinates, category (Neoplasm, Inflammation, Vascular...), confidence, dimensions, and anatomical location.
Asteroid Mode (optional)
Deep analysis combining results from all vision models, activating the Clinical Council (DeepSeek Reasoner) for advanced reasoning, generating clinical differentials, detailed dimensions, and prioritized clinical recommendations. Includes per-finding Deep Analysis.
Visualization + Chat + Report
Interactive bounding boxes over the image, findings panel with severity, PointAsk for focal questions, doctor's comment field, and PDF report generation — all in the browser.
Summary: 7 Cases, 20 Findings, Zero Critical Misses
| Case | Modality | Findings | Max. severity | Confidence |
|---|---|---|---|---|
| Pigmented macular lesion | Fundoscopy | 2 | Indeterminate | 95% |
| Multicentric retinoblastoma | Fundoscopy | 5 | Malignant | 98% |
| Papilledema | Fundoscopy | 1 | Suspicious | 98% |
| Ischemic retinopathy | Fundoscopy | 4 | Malignant | — |
| Hypoechoic mass 25×40 mm | Doppler US | 1 | Suspicious | 90% |
| Hypervascular superficial mass | Doppler US | 2 | Malignant | 95% |
| Complex cystic lesion | B-mode US | 1 | Indeterminate | 90% |
Who Is This For?
Primary care centers
General practitioners with portable retinal cameras or point-of-care ultrasound who need an instant second opinion before referring to a specialist.
Ophthalmology clinics
Automated fundus photograph screening to detect urgent pathology (papilledema, tumors, diabetic retinopathy) before the specialist reviews them.
Radiology departments
Musculoskeletal radiologists who want automated preliminary analysis of soft tissue Doppler ultrasounds, including measurements and clinical differential.
Telemedicine & rural areas
RADIA works in any browser. A rural doctor uploads an image and gets tertiary hospital-quality analysis. No installations, no VPNs, no specialized hardware.
Limitations & Responsibility
RADIA is a support tool, not a diagnosis
AI models make mistakes. Gemini, MedGemma, Llama, and DeepSeek are impressive but not infallible. That's why RADIA's workflow is explicit:
- The doctor reviews each AI-generated finding
- Can confirm, reject, or modify before including it in the report
- The "Doctor's comment" field adds clinical context the AI doesn't have
- The final report is signed by the professional, not the machine
AI serves as an exhaustive first read that reduces the probability of missed findings due to fatigue or volume, but the clinical decision always belongs to the professional.
One Platform, Any Clinical Image
RADIA started analyzing dental CTs. Today it processes fundus photographs that detect multicentric retinoblastoma and Doppler ultrasounds that differentiate hemangiomas from sarcomas. The same architecture — four AI models (3 vision + 1 reasoning), Cloudflare Workers, D1, edge analysis — adapts to any clinical image a professional needs analyzed.
What previously required specific desktop software, PACS licenses, and years of subspecialization is now available in a browser. A family doctor uploads a fundus photo taken with a portable retinal camera and gets analysis with bounding boxes, severity levels, clinical differentials, and referral recommendations — in seconds. That's real democratization of medical AI.
Next steps include support for dermatoscopy, obstetric ultrasound, digital mammography, and retinal OCT. The question is no longer whether AI can analyze medical imaging — it's how many specialties can be covered with this same approach.
Technologies in this article
🩻
Want to try it with your own images?
RADIA accepts DICOM, JPEG, PNG, and clinical photography from any modality. Upload a fundus image, an ultrasound, or a dental CT and get AI analysis in seconds.
Try RADIA